 --%3E%3Csvg version='1.1' id='Lager_1' xmlns='http://www.w3.org/2000/svg' xmlns:xlink='http://www.w3.org/1999/xlink' x='0px' y='0px' viewBox='0 0 1500 371.7' style='enable-background:new 0 0 1500 371.7%3B' xml:space='preserve'%3E%3Cstyle type='text/css'%3E.st0%7Bfill:%23005EA8%3B%7D%3C/style%3E%3Cg%3E%3Cpath class='st0' d='M237.9 12.6h-89.8v8.9l1.8 0.3c19.6 3 28.5 6.5 32 12.6c1.3 2.2 1.9 4.9 1.9 8.2c0 11.3-7.2 29.4-19 58.8c0 0-28.2 71.2-35.8 90.3c-3.6-9.2-47.8-121.4-47.8-121.4l-1.9-4.7c-3.2-8-6.8-16.7-6.8-24.1c0-3.1 0.6-5.9 2.1-8.4c3.6-6 12.5-9.8 26.3-11.3l1.9-0.2v-9H0v8.9l1.9 0.2c25.4 3 32.5 21.2 41.4 44.2l1 2.6c0 0 70.8 178.5 70.8 178.5h7.2l59.9-150.7l2.8-6.8c17.1-42.2 26.5-65.5 53-67.9l1.9-0.2v-9H237.9z'/%3E%3Cpath class='st0' d='M243.4 87.4l-40.9 14.9v6l1 0.6c18 11 18 14.4 18 27.3v63.2c-0.3 25.2-1 27.6-22.5 31l-1.8 0.3v8.9h76.7v-8.9l-1.8-0.3c-21.6-3.4-22.5-4.5-22.5-31V89.3l-5.5-2.1L243.4 87.4z'/%3E%3Cpath class='st0' d='M216.2 59.3c0 10.4 8.1 18.8 18 18.8c9.9 0 18-8.4 18-18.8c0-10.4-8.1-18.8-18-18.8C224.3 40.5 216.2 49 216.2 59.3'/%3E%3Cpath class='st0' d='M324.9 59.8h-3.7l-45.4 47.4l3.1 4.7h19.8v86.9c0 0 0 5.8 0 6.9c0 13.1 0.5 23.5 7.1 30.1c4.8 4.8 12.3 7.1 23.7 7.1c15.7 0 32.1-3.5 49.9-10.6l1.7-0.7l-2.2-9.2l-2.1 0.6c-5.3 1.5-11.3 2.2-17.8 2.2c-32.1 0-32.1-17.1-32.1-45.4v-68h49.1v-18H327V59.8H324.9z'/%3E%3Cpath class='st0' d='M433.7 87.4l-38.4 14.9v5.8l0.8 0.6c14.4 10.9 14.4 14.4 14.4 27.3v63.3c-0.3 25.2-0.9 27.6-20.9 31l-1.8 0.3v8.8h82v-8.9l-1.9-0.2c-29.2-3.5-29.2-5.6-29.2-31v-33.1l0-1.1c-0.3-17.4 2.2-46.8 22.4-48.8c5.2-0.5 11.7 4.9 16.5 8.8l3 2.4l1.2-0.6c8.4-4.2 17.3-13.1 17.3-22.5c0-10-7.6-17.2-18-17.2c-18.4 0-33.8 17.8-42.1 33.3c0.3-10.5 1-31.3 1-31.3l-5.6-2.1L433.7 87.4z'/%3E%3Cpath class='st0' d='M534.9 163.4c0-31.2 14.1-64.7 45.2-64.7c33.3 0 45.8 42.3 45.8 68.9c0 24.6-11.8 63.7-43.3 63.7C549.7 231.4 534.9 191.6 534.9 163.4 M501.7 165.7c0 45.4 32.3 77.1 78.6 77.1c44.1 0 78.7-34.4 78.7-78.4c0-45.4-32.2-77.1-78.3-77.1C535.7 87.3 501.7 121 501.7 165.7'/%3E%3Cpath class='st0' d='M710.6 0.3l-37.1 15V21l0.9 0.6c14.4 10.9 14.4 14.4 14.4 27.3v150.4c-0.3 25.2-1 27.6-22.5 31l-1.8 0.3v8.9h76.7v-8.9l-1.8-0.3c-21.6-3.4-22.5-4.5-22.5-31V2.1L711.4 0L710.6 0.3z'/%3E%3Cpath class='st0' d='M793.9 87.4L753 102.3v6l1 0.6c18 11 18 14.4 18 27.3v63.2c-0.3 25.2-1 27.6-22.5 31l-1.8 0.3v8.9h76.7v-8.9l-1.8-0.3c-21.6-3.4-22.5-4.5-22.5-31V89.3l-5.5-2.1L793.9 87.4z'/%3E%3Cpath class='st0' d='M766.7 59.3c0 10.4 8.1 18.8 18 18.8c9.9 0 18-8.4 18-18.8c0-10.4-8.1-18.8-18-18.8C774.7 40.5 766.7 49 766.7 59.3'/%3E%3Cpath class='st0' d='M868.3 36.2c-10.5 17.6-12.3 36.1-12.7 53.6c-1.8 1.1-25.3 15.4-25.3 15.4v6.6h25.2v87.6c-0.3 25.2-1 27.6-23.1 31l-1.8 0.3v8.9h82.9v-8.9l-1.9-0.2c-28-3.5-28-5.6-28-31v-87.6h40.4v-18h-40.4V76.3c0-23.1 3.2-61.7 24.9-61.7c14.2 0 27.4 17.4 32.5 24.9l0.6 0.9l1.1 0c6.2 0.2 11.5-1.5 15-4.8c2.9-2.8 4.4-6.5 4.4-11.1c0-17.8-23.4-24.4-38.2-24.4C902.7 0.2 881.9 13.7 868.3 36.2'/%3E%3Cpath class='st0' d='M987.7 98.7c14.1 0 22.2 14 25.3 28c-4.5 0.2-49.3 2.2-54.3 2.4C962.4 114.5 971.9 98.7 987.7 98.7 M925.2 168c0 42.7 29 74.8 67.4 74.8c23.1 0 45.7-15 59.1-39.1l0.9-1.6l-7.9-6.1l-1.3 1.8c-9.7 13.6-20.5 19.7-35 19.7c-14.5 0-27.2-5.5-36.9-16c-10.2-11-15.9-26.2-15.9-42.5c0-1.7 0.1-3.4 0.2-5.1c0 0 0.9-11.4 1.1-14.4h90.5l-0.1-2.2c-1.3-30.5-20.9-50.2-50-50.2C956.2 87.3 925.2 122 925.2 168'/%3E%3Cpath class='st0' d='M1436.4 173.1c0.6-90.8 69.3-98.9 63.2-133.3c-7.7-43.9-149-57.6-253.8-9.8c-36 16.4-67.6 33.7-98.5 57.3c-7.3 5.8-9.5 12.6-10 19.2c0.5 38.6 11.9 74.6 31.1 105.1c6-8.3 12.5-17 18.6-25.1c19.6-25.8 23.2-31.2 57.9-58.8c69.5-55.2 178.1-83.1 186.1-59.1c7.9 23.8-37.2 42.7-37.2 107.2c0 43.2 21.1 73.5 39.6 91.8v0c11 9.9 14.9 6.4 22.3 2.1c0.5-0.3 1-0.5 1.4-0.6c13-9.2 24.9-20 35.4-31.9C1459.4 223.9 1436.2 205 1436.4 173.1'/%3E%3C/g%3E%3Cg%3E%3Cpolygon points='950.2 360.9 937.6 329.4 930.1 329.4 947.5 370.8 952.7 370.8 970.1 329.4 962.7 329.4 '/%3E%3Crect x='980.2' y='329.4' width='6.6' height='41.5'/%3E%3Cpolygon points='994.8 335.2 1006.1 335.2 1006.1 370.8 1012.7 370.8 1012.7 335.2 1024 335.2 1024 329.4 994.8 329.4 '/%3E%3Cpath d='M1056.4 351.5c1.5-1.1 2.6-2.5 3.4-4.2c0.8-1.7 1.2-3.6 1.2-5.7c0-2.5-0.6-4.7-1.7-6.6c-1.1-1.8-2.7-3.2-4.8-4.2c-2-1-4.5-1.5-7.2-1.5h-12.9v41.5h6.6v-16.3h2.9l12.4 16.3h8.3l-13.6-17C1053.1 353.4 1054.9 352.6 1056.4 351.5z M1045.4 349h-4.4v-14.4h4.4c2.8 0 4.9 0.6 6.5 1.9c1.5 1.3 2.3 3 2.3 5.3c0 1.5-0.4 2.8-1.1 3.9c-0.7 1.1-1.7 1.9-3 2.5C1048.8 348.7 1047.2 349 1045.4 349z'/%3E%3Cpath d='M1107 334.9c-1.9-2-4.1-3.5-6.7-4.6c-2.5-1.1-5.2-1.7-8.1-1.7c-2.9 0-5.6 0.6-8.1 1.7c-2.5 1.1-4.7 2.6-6.7 4.6c-1.9 2-3.4 4.3-4.5 6.9c-1.1 2.6-1.6 5.4-1.6 8.4c0 3 0.5 5.8 1.6 8.4c1.1 2.6 2.6 4.9 4.5 6.9c1.9 2 4.1 3.5 6.7 4.6c2.5 1.1 5.2 1.7 8.1 1.7c2.9 0 5.6-0.6 8.1-1.7c2.5-1.1 4.8-2.6 6.7-4.6c1.9-2 3.4-4.3 4.5-6.9c1.1-2.6 1.6-5.4 1.6-8.4c0-3-0.5-5.8-1.6-8.4C1110.4 339.1 1108.9 336.9 1107 334.9z M1105 356.2c-0.7 1.9-1.7 3.5-2.9 4.8c-1.2 1.4-2.7 2.4-4.4 3.2c-1.7 0.8-3.5 1.1-5.5 1.1c-2 0-3.8-0.4-5.5-1.1s-3.1-1.8-4.4-3.2c-1.2-1.4-2.2-3-2.9-4.8c-0.7-1.9-1-3.9-1-6c0-2.2 0.3-4.2 1-6c0.7-1.8 1.7-3.4 2.9-4.8s2.7-2.4 4.4-3.2c1.7-0.8 3.5-1.1 5.5-1.1c2 0 3.8 0.4 5.5 1.1c1.7 0.8 3.2 1.8 4.4 3.2c1.2 1.4 2.2 3 2.9 4.8c0.7 1.8 1 3.9 1 6C1106 352.3 1105.6 354.3 1105 356.2z'/%3E%3Cpolygon points='1131.7 329.4 1125.1 329.4 1125.1 370.8 1147.5 370.8 1147.5 365.1 1131.7 365.1 '/%3E%3Crect x='1158' y='329.4' width='6.6' height='41.5'/%3E%3Cpolygon points='1179.4 370.8 1186 370.8 1186 353 1200.8 353 1200.8 347.2 1186 347.2 1186 335.2 1201.9 335.2 1201.9 329.4 1179.4 329.4 '/%3E%3Cpolygon points='1213.6 370.8 1235.9 370.8 1235.9 365.1 1220.2 365.1 1220.2 353 1235.3 353 1235.3 347.2 1220.2 347.2 1220.2 335.2 1235.9 335.2 1235.9 329.4 1213.6 329.4 '/%3E%3Cpath d='M1282.6 354.2h12.5v0.9c0 1.6-0.3 3-1 4.3c-0.7 1.3-1.6 2.4-2.7 3.3c-1.1 0.9-2.4 1.7-3.9 2.2c-1.4 0.5-2.9 0.8-4.5 0.8c-1.9 0-3.7-0.4-5.3-1.2c-1.6-0.8-3.1-1.9-4.3-3.3c-1.2-1.4-2.2-3.1-2.9-5c-0.7-1.9-1-4-1-6.3c0-2.1 0.3-4.1 0.9-6c0.6-1.9 1.5-3.5 2.7-4.9c1.2-1.4 2.6-2.5 4.3-3.3c1.7-0.8 3.7-1.2 5.9-1.2c2.3 0 4.5 0.4 6.7 1.3c2.2 0.9 4 2 5.5 3.6l3.2-5.1c-1.3-1.2-2.8-2.2-4.5-3.1c-1.7-0.8-3.4-1.5-5.3-1.9c-1.9-0.4-3.8-0.7-5.7-0.7c-3.2 0-6.1 0.6-8.7 1.7c-2.6 1.2-4.8 2.7-6.6 4.7c-1.8 2-3.2 4.3-4.2 6.9c-1 2.6-1.4 5.3-1.4 8.2c0 3.1 0.5 5.9 1.6 8.5c1 2.6 2.5 4.9 4.3 6.9c1.9 2 4 3.5 6.5 4.6c2.5 1.1 5.1 1.6 8 1.6c2.4 0 4.7-0.4 7-1.2c2.3-0.8 4.3-1.9 6.1-3.4c1.8-1.5 3.3-3.3 4.3-5.5c1.1-2.1 1.6-4.5 1.6-7.2V349h-19.2V354.2z'/%3E%3Cpath d='M1335.6 351.5c1.5-1.1 2.6-2.5 3.4-4.2c0.8-1.7 1.2-3.6 1.2-5.7c0-2.5-0.6-4.7-1.7-6.6c-1.1-1.8-2.7-3.2-4.8-4.2c-2-1-4.5-1.5-7.2-1.5h-12.9v41.5h6.6v-16.3h2.9l12.4 16.3h8.3l-13.6-17C1332.3 353.4 1334.1 352.6 1335.6 351.5z M1324.6 349h-4.4v-14.4h4.4c2.8 0 4.9 0.6 6.5 1.9c1.5 1.3 2.3 3 2.3 5.3c0 1.5-0.4 2.8-1.1 3.9c-0.7 1.1-1.7 1.9-3 2.5C1328 348.7 1326.4 349 1324.6 349z'/%3E%3Cpath d='M1386.2 334.9c-1.9-2-4.1-3.5-6.7-4.6c-2.5-1.1-5.2-1.7-8.1-1.7c-2.9 0-5.6 0.6-8.1 1.7c-2.5 1.1-4.7 2.6-6.7 4.6c-1.9 2-3.4 4.3-4.5 6.9c-1.1 2.6-1.6 5.4-1.6 8.4c0 3 0.5 5.8 1.6 8.4c1.1 2.6 2.6 4.9 4.5 6.9c1.9 2 4.1 3.5 6.7 4.6c2.5 1.1 5.2 1.7 8.1 1.7c2.9 0 5.6-0.6 8.1-1.7c2.5-1.1 4.8-2.6 6.7-4.6c1.9-2 3.4-4.3 4.5-6.9c1.1-2.6 1.6-5.4 1.6-8.4c0-3-0.5-5.8-1.6-8.4C1389.6 339.1 1388.1 336.9 1386.2 334.9z M1384.2 356.2c-0.7 1.9-1.7 3.5-2.9 4.8c-1.2 1.4-2.7 2.4-4.4 3.2s-3.5 1.1-5.5 1.1c-2 0-3.8-0.4-5.5-1.1s-3.1-1.8-4.4-3.2c-1.2-1.4-2.2-3-2.9-4.8c-0.7-1.9-1-3.9-1-6c0-2.2 0.3-4.2 1-6c0.7-1.8 1.7-3.4 2.9-4.8c1.2-1.4 2.7-2.4 4.4-3.2c1.7-0.8 3.5-1.1 5.5-1.1c2 0 3.8 0.4 5.5 1.1c1.7 0.8 3.2 1.8 4.4 3.2c1.2 1.4 2.2 3 2.9 4.8c0.7 1.8 1 3.9 1 6C1385.2 352.3 1384.9 354.3 1384.2 356.2z'/%3E%3Cpath d='M1427.6 354.3c0 3.8-0.7 6.6-2.1 8.3c-1.4 1.7-3.6 2.6-6.6 2.6c-3 0-5.2-0.9-6.6-2.6c-1.4-1.7-2.1-4.5-2.1-8.3v-24.9h-6.6v26.7c0 5.1 1.3 9 3.9 11.6c2.6 2.6 6.4 3.9 11.4 3.9c5.1 0 8.9-1.3 11.4-3.9c2.6-2.6 3.8-6.5 3.8-11.6v-26.7h-6.6V354.3z'/%3E%3Cpath d='M1468.5 330.8c-2.1-0.9-4.4-1.4-7.1-1.4h-12.9v41.5h6.6v-16.5h6.3c2.7 0 5.1-0.5 7.1-1.5c2.1-1 3.7-2.5 4.8-4.4c1.2-1.9 1.7-4.2 1.7-6.8c0-2.7-0.6-4.9-1.7-6.7C1472.1 333.1 1470.5 331.7 1468.5 330.8z M1467 345.8c-0.8 1.1-1.8 1.9-3.1 2.4c-1.3 0.5-2.8 0.8-4.5 0.8h-4.4v-14.4h4.4c1.7 0 3.1 0.3 4.5 0.8c1.3 0.5 2.4 1.3 3.1 2.4c0.8 1.1 1.2 2.4 1.2 4C1468.2 343.4 1467.8 344.8 1467 345.8z'/%3E%3Cpolygon points='1492.3 329.4 1490.8 329.4 1489 334.3 1487.1 329.4 1485.7 329.4 1484.9 336.9 1486.3 336.9 1486.8 331.8 1488.6 336.7 1489.4 336.7 1491.2 331.8 1491.7 336.9 1493 336.9 '/%3E%3Cpolygon points='1479.5 330.6 1481.4 330.6 1481.4 336.9 1482.8 336.9 1482.8 330.6 1484.7 330.6 1484.7 329.4 1479.5 329.4 '/%3E%3Cpath d='M664.5 370.9v-41.6h10.8c2.7 0 5.1 0.5 7.1 1.4c2 0.9 3.5 2.3 4.6 4c1.1 1.7 1.6 3.8 1.6 6.3c0 2.4-0.5 4.6-1.6 6.4c-1.1 1.8-2.6 3.3-4.6 4.3c-2 1-4.3 1.5-7.1 1.5h-7v17.6H664.5z M668.3 350.1h6c2.1 0 3.9-0.4 5.4-1.1c1.5-0.7 2.7-1.8 3.6-3.1c0.8-1.3 1.3-2.9 1.3-4.7c0-1.8-0.4-3.4-1.3-4.7c-0.8-1.3-2-2.3-3.6-3c-1.5-0.7-3.3-1-5.4-1h-6V350.1z'/%3E%3Cpath d='M694.4 370.9l16.4-41.6h3.6l16.3 41.6h-4.1l-5.1-13.2h-17.9l-5.1 13.2H694.4z M705 354.3h15.3l-7.6-19.9L705 354.3z'/%3E%3Cpath d='M743 370.9v-41.6h10.8c2.7 0 5.1 0.5 7.1 1.4c2 0.9 3.5 2.3 4.6 4c1.1 1.8 1.6 3.9 1.6 6.3c0 2.2-0.5 4.2-1.4 5.9c-0.9 1.7-2.2 3.1-3.9 4.1c-1.7 1-3.7 1.7-6 1.9l13.8 17.9h-4.9l-13.2-17.5h-4.7v17.5H743z M746.8 350.1h6c2.1 0 3.9-0.4 5.5-1.1c1.5-0.7 2.7-1.8 3.5-3.1c0.8-1.3 1.2-2.9 1.2-4.7c0-2.7-0.9-4.9-2.7-6.4c-1.8-1.5-4.3-2.3-7.5-2.3h-6V350.1z'/%3E%3Cpath d='M787.7 370.9v-38.1H775v-3.5h29.2v3.5h-12.7v38.1H787.7z'/%3E%3Cpath d='M850.7 371.7c-2.9 0-5.6-0.6-8.2-1.7c-2.5-1.1-4.8-2.6-6.7-4.6c-1.9-2-3.4-4.3-4.5-6.9c-1.1-2.6-1.6-5.4-1.6-8.4c0-3 0.5-5.8 1.6-8.4c1.1-2.6 2.6-4.9 4.5-6.9c1.9-2 4.1-3.5 6.7-4.6c2.5-1.1 5.3-1.7 8.2-1.7c2.9 0 5.6 0.6 8.2 1.7c2.5 1.1 4.8 2.6 6.7 4.6c1.9 2 3.4 4.3 4.5 6.9c1.1 2.6 1.6 5.4 1.6 8.4c0 3-0.5 5.8-1.6 8.4c-1.1 2.6-2.6 4.9-4.5 6.9c-1.9 2-4.1 3.5-6.7 4.6C856.3 371.2 853.6 371.7 850.7 371.7z M850.7 368c2.4 0 4.6-0.5 6.6-1.4c2-0.9 3.8-2.2 5.4-3.8c1.5-1.6 2.7-3.5 3.6-5.7c0.9-2.2 1.3-4.5 1.3-7s-0.4-4.8-1.3-7c-0.9-2.2-2.1-4.1-3.6-5.7c-1.5-1.6-3.3-2.9-5.4-3.8c-2-0.9-4.2-1.4-6.6-1.4s-4.6 0.5-6.6 1.4c-2 0.9-3.8 2.2-5.4 3.8c-1.5 1.6-2.7 3.5-3.6 5.7c-0.9 2.2-1.3 4.5-1.3 7s0.4 4.8 1.3 7c0.9 2.2 2.1 4.1 3.6 5.7c1.5 1.6 3.3 2.9 5.4 3.8C846.1 367.6 848.3 368 850.7 368z'/%3E%3Cpolygon points='906.4 332.7 906.4 329.4 885.4 329.4 885.4 370.9 889.2 370.9 889.2 351.8 905.3 351.8 905.3 348.4 889.2 348.4 889.2 332.7 '/%3E%3C/g%3E%3C/svg%3E)
This blog focuses on EmbryoGlue® as there are now three Cochrane reviews showing improved clinical outcome when using this transfer medium, which contains a functional concentration of hyaluronan. The Number Needed to Treat (number of patients treated with EmbryoGlue to achieve an additional live birth) is reported to be around 17 patients, so perhaps the use of this specifically created transfer medium should not be considered an add-on, but rather a standard of care.
Development of a specific medium for embryo transfer
The concentration of the macromolecule hyaluronan, is known to increase in the uterus around the time of implantation (Carson et al., 1987; Zorn et al., 1995; Salamonsen et al., 2001). When included in culture and/or transfer media it was shown to increase mouse embryo implantation and fetal development rates (Gardner et al., 1999). Consequently, EmbryoGlue was developed by adding 0.5mg/ml recombinant hyaluronan to a G-2 medium backbone and replacing human serum albumin with recombinant human albumin. G-2 was used as it mimics conditions in the uterus and fulfils embryo nutritional requirements of the post-compaction stages. Recombinant albumin was utilised to avoid having a blood derived product in the transfer medium. It also removed the inherent variation between human serum albumin LOTS. Furthermore, as with the comparison of recombinant and urinary derived gonadotropins, if efficacy is the same it is not surprising that patients would prefer a medical device that is introduced into their body to not be human derived.
How might hyaluronan promote implantation?
The exact mechanism(s) by which EmbryoGlue facilitates implantation and improves clinical outcomes is not fully understood. It is plausible that having a similar concentration of hyaluronan in the transfer medium to that of the uterine secretions could aid transition and apposition of the embryo. One clear physical effect of the high functional concentration of hyaluronan in EmbryoGlue is the increased viscosity and miscibility compared to standard culture media. Interestingly, it is well known that the uterine milieu is also characterised by a high viscosity. A recent study simulated the intrauterine mixing flow between the uterine milieu and the transfer medium (Ding et al., 2018). Based on their computational results the authors recommended the use of a high viscosity transfer medium in combination with a slow injection speed. The potential contribution of high viscosity in EmbryoGlue to better clinical outcomes has only partly been studied (Reed and Said, 2019) and may deserve more attention in future studies.
The hyaluronan in EmbryoGlue may also act to promote cell adhesion. For example, a cell surface receptor (CD44) that binds to hyaluronan is present on the human blastocyst (Campbell et al., 1995) and stromal cells of the endometrium (Yaegashi et al., 1995). One recent study using human embryos donated for research was able to show that the receptor for hyaluronan is present at all stages of human embryo development, with a slightly higher expression at the blastocyst stage (Ruane et al., 2020). A high level of blastocyst attachment was not further enhanced by EmbryoGlue in the in vitro model using endometrial endothelial cells. However, it is still unclear if this is also the situation in vivo. The presence of the hyaluronan receptors suggest a role for attachment, but there are potentially other or additional mechanisms, for example, promotion of gene expression and embryo growth.
The break-through of EmbryoGlue in IVF
EmbryoGlue is almost two decades old, but it was actually developed and tested in line with a process described by Harper and colleagues in 2012. Following the initial mouse studies, the first prospective study in humans evaluated the effect on implantation of high levels of hyaluronan in an embryo transfer medium, by adding hyaluronan to G-2 (Schoolcraft et al., 2002). This study demonstrated increased implantation rates after transfer of day 3 embryos. Subsequently, EmbryoGlue was developed and launched as a commercial product in 2003. The first two randomised control trials using this product were by Valojerdi et al., (2006) and Freidler et al., (2007). The first study randomised day 3 transfers in 815 patients into EmbryoGlue or G-1 containing recombinant albumin. EmbryoGlue significantly increased live birth rates. Freidler et al., investigated day 2 and 3 transfers in a select group of patients (<43 years old with repeated implantation failure). EmbryoGlue was compared to HTF supplemented with 20% SSS for transfer. Significant increases in implantation rate, clinical pregnancy rate and delivered/ongoing pregnancy rate were observed following transfer with EmbryoGlue. The study was stopped after half of the patients had been randomised as the difference had exceeded the proposed improvement.
A larger study with >600 transfers in each group was completed by Urman et al., (2008). EmbryoGlue was compared to G-2 PLUS for transfer (Note: G-2 already contains 0.125mg/ml hyaluronan). A significant increase was observed in both implantation and clinical pregnancy rates. Interestingly, the beneficial influence of EmbryoGlue was more evident in women >35 years old, those with previous failed cycles or with poor quality embryos. The Number Needed to Treat (NNT) is defined as the number of patients who must be treated to cause a single occurrence of a positive outcome of interest. The table below provides a series of NNT calculation based on the data by Urman et al., (2008) and shows how many patients are potentially required in each group to achieve one additional pregnancy. A follow up study by Urman and colleagues (Balaban et al., 2011) showed that the EmbryoGlue patients from the 2008 study also had significantly higher live birth rates. The number of children born per number of embryos transferred was also significantly higher.
In addition, a retrospective study with 743 embryos, implantation, clinical pregnancy and delivery rates were all statistically higher when performed with EmbryoGlue (Sun et al., 2010). The NNT was calculated as 15, which is similar to that reported by Urman et al., (2008). As a reference, the NNT for avoiding infection at the site of a compound fracture using antibiotics is 16 (Gosselin et al., 2004), which means 1 in 16 patients avoided infection with preventative antibiotics. Would you want to take a course of antibiotics following such an incident? This is the very reason why it is standard clinical practice to provide antibiotics in such a scenario.
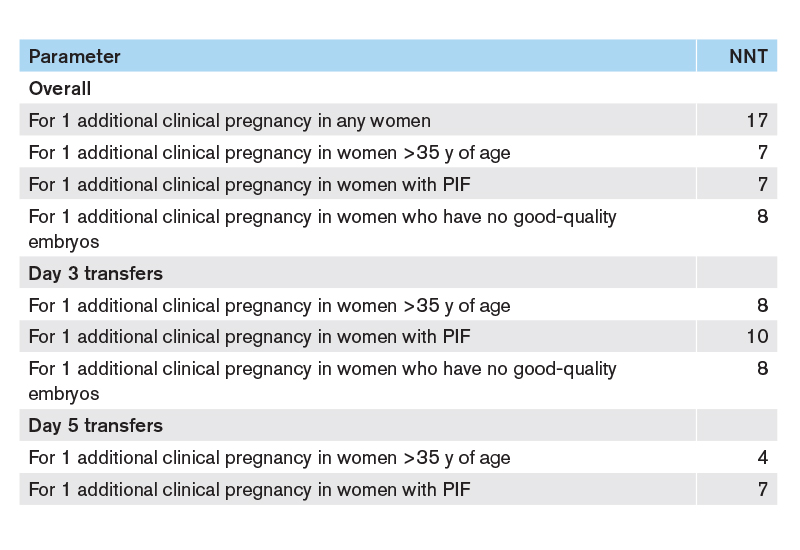
This Table shows the Numbers Needed to Treat (NNT) to get one additional clinical pregnancy for the total patient group and for subgroups using EmbryoGlue for embryo transfer (Urman et al., 2008). PIF = Previous implantation failure.
Benefits with EmbryoGlue inspired further clinical validations
In a study with a total of 224 patients a clinically relevant 6% increase in ongoing pregnancy rate was reported by Hazlett et al., (2008), but the study was powered to show an ambitious 20% increase. This demonstrates one of the main challenges when an end point is a clinical outcome. To detect a single digit, but clinically relevant increase, the study would need at least 4 times more patients. In a prospective observational study, Hambiliki et al., (2010), showed a significant increase in biochemical and implantation rates, but no increase in clinical pregnancy rate. Although it is difficult to draw a conclusion from this study as more embryos were transferred in the control group, but the study group received more high grade embryos.
The first meta-analysis was performed in 2010 by the Cochrane collaboration, followed by an update in 2014 (Bontekoe et al., 2010, 2014). The updated Cochrane review was based on seventeen studies using high hyaluronan in almost 4000 embryo transfers. The report concluded that the evidence suggests improved clinical pregnancy and live birth rates when hyaluronan is used at a high, functional concentration compared to low or no hyaluronan. The evidence by many studies was deemed of moderate quality according to GRADE working group criteria. However, the study with the largest patient population (mentioned above: Balaban et al., 2011) was classified with low risk of bias. During the same time period of the two initial Cochrane reports, numerous studies on EmbryoGlue were performed in Japan. This resulted in a meta-analysis on 23 studies with almost 10,000 embryo transfer cycles, which were performed with or without EmbryoGlue and either fresh or frozen embryo transfer (Hashimoto et al., 2014). Significantly higher implantation and clinical pregnancy rates were obtained with both fresh and frozen transfer cycles with EmbryoGlue.
In 2017 Harper et al., reviewed the evidence of adjuncts in the laboratory. Their conclusion on EmbryoGlue was that “published evidence may be suggestive of a beneficial effect but further RCTs are required”. Since the publication of this opinion and the first two Cochrane reviews numerous other studies have been reported. A RCT on 772 frozen blastocyst transfer cycles reported significantly higher clinical pregnancy and live birth rates by using EmbryoGlue (Tan et al., 2017*). Significantly higher ongoing pregnancy rates following frozen embryo transfers was also reported in a smaller retrospective study by Charulata et al., (2017). Flouri et al., (2017) showed in a retrospective study with matched controls, a statistical increase in implantation, clinical pregnancy and live birth rates with 234 patients when using EmbryoGlue. Another randomised trial investigated the impact of the day of transfer in fresh transfer cycles on day 2, 3, 4 and 5 with almost 500 patients (Zborilova et al., 2018). Clinical pregnancy rates were always higher in the study group. The absolute differences between the treatment groups were almost 10% higher on day 4 and day 5 transfer cycles compared to 5-7% for days 2 and 3. Wang et al., (2019), performed a retrospective comparison of 476 transfers with G-2 PLUS to 161 transfers with EmbryoGlue. The study showed a significant increase in implantation and clinical pregnancy rate with EmbryoGlue. Delivery rate was also higher, but did not quite reach significance (p = 0.057).
Santos Simões et al., (2019) showed that patients with polycystic ovary syndrome (PCOS) exhibit a significant reduction in the synthesis of hyaluronic acid and a reduced expression of hyaluronic acid Synthase 3 in their endometrium. Interestingly, Kandari et al., (2019) showed in a RCT that embryo transfer using EmbryoGlue in PCOS patients resulted in a significant increase in implantation and live birth rates compared to a transfer medium without hyaluronan.
Latest Cochrane update expanded with new studies
Because of the increase in published studies, in September 2020 the Cochrane review was updated with 7 new studies (Heymann et al., 2020). The new analysis incorporates 26 studies involving 6704 participants. With a moderate level of evidence the conclusion was that compared to no or a low level of hyaluronan, EmbryoGlue would probably increase live birth rate. This conclusion was based on 10 RCTs involving 4066 participants. Assuming the chance of a live birth is 33% with no/low hyaluronan the chance with EmbryoGlue would be between 37-44%. This translates into 1 additional live birth for every 14 embryos transferred, which is similar to that reported by Urman et al., (2008) and Sun et al., (2010). Furthermore, with the additional data the odds ratio for live birth has now increased to 1.35.
A single product is not going to be a panacea
The IVF process is complicated, with many confounding factors. Thus, it is perhaps unsurprising that a product used at the final in vitro stage (embryo transfer) does not demonstrate a significant improvement in every situation (Loutradi et al., 2007; Fancsovits et al., 2015; Chun et al., 2016; Fu et al., 2018; Yung et al., 2019). EmbryoGlue should not be considered a panacea. It is not going to rescue an embryo that has been cultured under suboptimal conditions. For example, Fancsovits et al., (2015) reported no difference in clinical outcomes between embryos transferred in EmbryoGlue or G-2 PLUS, but in this study embryos were cultured in atmospheric oxygen, a known cellular stressor.
There are, in fact, only two studies that reported a decrease in clinical outcomes (Morbeck et al., 2007, Ebrahimi Ghaei et al., 2020). The RCT by Morbeck et al., was terminated early due to lower implantation rates in the study group. The study by Ebrahimi Ghaei et al., was a retrospective evaluation of data collected over a five year period and showed a negative effect of extended exposure to EmbryoGlue (> 30 mins) with an implantation rate in the long exposure group that was less than half that of the short exposure group (15.6% versus 36.7%). The cause of the lower implantation rate in both studies is unknown, however, it is important to note that EmbryoGlue is based on the G-2 medium formulation, so there is no fundamental reason that the medium would cause detrimental results.
Although Wang et al., (2019) also reported that a longer exposure time (> 60 minutes) could negatively impact the clinical outcome results this is not always the case. A meta analysis of 19 studies demonstrated increased implantation rates with exposure times >30 minutes (Gkotsi et al., 2021). Furthermore , no significant difference was observed between exposure times of >30 and >60 minutes. In another study where blastocysts were cultured in EmbryoGlue for different incubation times prior transfer, it was found that clinical outcomes increased with longer exposure times (0.5, 1, 2 and 3 hours: Perez et al., 2019). This result is supported by a mouse study where embryos were incubated for 1 hour or 4 hours. Embryos transferred after 4 hours of incubation in EmbryoGlue resulted in a higher number of implantations resulting in a fetus compared to the control and embryos exposed for 1 hour*.
Considerations for dish set-up when using EmbryoGlue
Preparation of the dishes is an important consideration and might provide an explantation for the discrepancy with longer exposure times. It is common practice in some laboratories to prepare the transfer dish on the day of transfer using either fresh or pre-equilibrated medium. When using EmbryoGlue that has been pre-equilibrated in, for example, a tube, a change can occur in both temperature and pH while being dispensed into a dish. Inappropriate pH and/or temperature may have a detrimental effect on the embryo. Further, osmolality changes may occur if the medium is equilibrated in an incubator/dish with suboptimal conditions. If the osmolality has increased this could also explain why some studies have seen a negative impact from long exposure times with EmbryoGlue.
The most documented embryo transfer medium
Since the introduction of EmbryoGlue in 2003 there has been mounting clinical evidence that it increases both clinical pregnancy and live birth rates. Due to the numerous confounding factors within an IVF cycle it should not, however, be considered a panacea, as it cannot necessarily make up for suboptimal laboratory procedures. However, given the significant number of publications outlined above, and the reported Number Needed to Treat to achieve one additional pregnancy, it clearly demonstrates that EmbryoGlue should be considered as a standard of care embryo transfer medium.
Summary of selected studies using EmbryoGlue
Are you interested in learning more about EmbryoGlue? Download this booklet where some of the significant number of studies on EmbryoGlue have been summarised. The studies are looking at the benefits of EmbryoGlue when used for different patient groups.

References
Balaban B, Yakin K, Ata A, Isiklar A, Urman B (2011) Effect of hyaluronan take home baby rate after day 3 and day 5 embryo transfers; a prospective randomized study. Hum Reprod 26 Supp1 i24.
Bontekoe S, Blake D, Heineman MJ, Williams EC, Johnson N (2010) Adherence compounds in embryo transfer media for assisted reproductive technologies. Cochrane Database Syst Rev (7) CD007421.
Bontekoe S, Johnson N, Blake D (2014) Adherence compounds in embryo transfer media for assisted reproductive technologies. Cochrane Database Syst Rev (2) CD007421.
Campbell S, Swann HR, Aplin JD, Seif MW, Kimber SJ, Elstein M (1995) CD44 is expressed throughout pre-implantation human embryo development. Hum Reprod 10 (2) 425-430.
Carson DD, Dutt A, Tang JP (1987) Gycoconjugate synthesis during early pregnancy: hyaluronate synthesis and function. Dev Biol 120 228-235.
Charulata C, Mantravadi K, Rao DG. (2017) Hyaluronan enriched transfer media improves reproductive outcomes in frozen thawed cycles for couples with repeatewd implantation failure. Hum Reprod 32 Suppl1 i238-239.
Chun S, Seo JE, Rim YJ, Joo JH, Lee YC, Koo YH (2016) Efficacy of hyaluronan-rich transfer medium on implantation and pregnancy rates in fresh and frozen-thawed blastocyst transfers in Korean women with previous implantation failure. Obstet Gynecol Sci 59 (3) 201-207.
Ding D, Shi W, Shi Y (2018) Numerical simulation of embryo transfer: how the viscosity of transferred medium affects the transport of embryos. Theor Biol Med Model 15 20
Ebrahimi Ghaei R, Harrity C, Riordan C, Moran C, Keane D (2020) Duration of exposure to EmbryoGlue (EG) may significantly impact implantation and clinical pregnancy rates following Embryo Transfer (ET). Hum Reprod 35 Suppl 1 i259-i260
Flouri C, Tailor S, Vourliotis M, Francis G, Papoff F, Sotircho G, Almeida P (2017) The effect of EmbryoGlue on clinical outcome. Fertility P-179, Edinburgh, UK
Fancsovitz P, Lehner A, Murber A, Kaszas Z, Rigo J, Urbancsek J (2015) Effect of hyaluronan-enriched embryo transfer medium on IVF outcome: a prospective randomized clinical trial. Arch Gynecol Obstet 291 1173-1179.
Friedler S, Schachter M, Strassburger D, Esther K, Ron ER, Raziel A (2007) A randomized clinical trial comparing recombinant hyaluronan/recombinant albumin versus human tubual fluid for cleavage stage embryo transfer in patients with multiple IVF-embryo transfer failure. Hum Reprod 22 (9) 2444-2448.
Fu W, Yu M, Zhang XJ (2018) Effect of hyaluronic acid-enriched transfer medium on frozen-thawed embryo transfer outcomes. J Obstet Gynaecol Res 44 (4) 747–755.
Gardner DK, Rodriguez-Martinez H, Lane M (1999) Fetal development after transfer is increased ny replacing protein with the gycosaminoglycan hyaluron for mouse embryo culture and transfer. Hum Reprod 14 2575-2580.
Gosselin RA, Roberts I, Gillespie WJ (2004) Antibiotics for preventing infection in open limb fractures. Cochrane Database Syst Rev (1) CD003764.
Harper J, Magli MC, Lundin K, Barratt CL, Brison D (2012) When and how should new technology be introduced into the IVF laboratory? Hum Reprod 27 303-313.
Harper J, Jackson E, Sermon K, Aitken RJ, Harbottle S, Mocanu E, Hardarson T, Mathur R, Viville S, Vail A, Lundin K (2017) Adjuncts in the IVF laboratory: where is the evidence for add-on interventions? Hum Reprod 32 485-491.
Hambiliki F, Ljunger E, Karlstrom PO, Stavreus-Evers A (2010) Hyaluronan-enriched transfer medium in cleavage-stage frozen-thawed embryo transfers increases implantations rate without improvement of delivery rate. Fert Steril 94 (5) 1669-1673.
Hashimoto et al. (2014) EmbryoGlue improves pregnancy and implantation rates: results from a meta-analysis on almost 10000 embryo transfers. Abstracts of the 10th Biennal Conference of Alpha; Scientists in Reproductive Medicine S7-S8 pp-009.
Hazlett WD, Meyer LR, Nasta TE, Mangan PA, Karande VC (2008) Impact of EmbryoGlue as the embryo transfer medium. Fert Steril 90 (1) 214-216.
Heymann D, Vidal L, Or Y, Shoham Z (2020) Hyaluronic acid in embryo transfer media for assisted reproductive technologies. Cochrane Database Syst Rev 9 CD007421.
Kandari S (2019) Time lapse selected elective single embryo transfer in hyaluronan enriched transfer medium in PCOS improves life birth rates compared to use of conventional embryo transfer media. A possible alternative to freeze-all cycles in PCOS. Fertil Steril 112 (3) Suppl e47.
Loutradi KE,Prassas I, Bili E, Sanopoulou T, Bontis I, Tarlatzis BC (2007) Evaluation of a transfer medium containing high concentration of hyaluronan in human in vitro fertilization. Fert Steril 87 (1) 48-52.
Morbeck et al. (2007) Prospective randomized clinical trial of novel implantation promoting medium (EmbryoGlue) to improve IVF success rates. [NTC00588250]. Clinical Trials Gov.
Perez O, Adriaanse H, Tilley B, Navarrete G, Lay L, Little LM, Gada R, Lawrence L, Lee K, Thomas MR, et al. (2019) The effect of extended blastocyst exposure of hyaluronan enriched transfer media on implantation rate in frozen embryo transfers. Fertil Steril 112 (3) Suppl e438.
Reed ML, Said AH (2019) Estimation of embryo transfer media viscosity and considerations of its effect on media and uterine fluid interactions. Reprod Biomed Online 39 931-939.
Ruane PT, Buck CJ, Babbington PA, Aboussahoud W, Berneau SC, Westwood M, Kimber SJ, Aplin JD, Brison DR (2020) The effects of hyaluronate-containing medium on human embryo attachment to endometrial epithelial cells in vitro. Hum Reprod Open 28 hoz033.
Salamonsen LA, Shuster S, Stern R (2001) Distribution of hyaluron in human endometrium across the menstrual cycle. Implications for implantationa and menstruation. Cell Tissue Res 306 335-340.
Schoolcraft W, Lane M, Stevens J, Gardner DK (2002) Increased hyaluronan concentration in the embryo transfer medium results in significant increase in human embryo implantation rate. Fertil Steril 76 Suppl 3 S5.
Santos Simões R, Carbonel AAF, Borges FT, Baracat MCP, da Silva Sasso GR, Simões MJ, Serafini PC, Soares JM Júnior, Nader HB, Baracat EC. (2019) Analysis of hyaluronic acid in the endometrium of women with polycystic ovary syndrome. Gynecol Endocrinol. 35 (2) 133-137.
Sun HX, Hu YL, Wang B (2010) A retrospective clinical study on effects of hyaluronan-containing transfer medium on implantation, pregnancy and delivery. J Reproduktionsmed Endokrinol 7:M-036
Urman B, Yakin K, Ata A, Isiklar A, Balaban B (2008) Effect of hyaluronan-enriched transfer medium on implantation and pregnancy rates after day 3 and day 5 embryo transfers: a prospective randomized study. Fertil Steril 90 604-612.
Valojerdi MR, Karimian L, Yazdi PE, Gilani MA, Madani T, Baghestani AR (2006) Efficacy of a human embryo transfer medium: a prospective, randomized clinical trial study. J Assist Reprod and Genet 23 (5) 207-212.
Wang W, Ren L, Wie D, Shen Y, Liu B, Wang Y, Chen F, Li M, Yan L, Feng Z, Shang W (2019) Effect of maternal and embryonic factors on frozen-thawed IVF-ET outcome after pre-equilibration with hyaluronan. Arch Gynecol Obstet 299 247-258.
Yaegashi N, Fujita N, Yajima A, Nakamura M (1995) Menstrual cycle dependent expression of CD44 in normal human endometrium. Hum Pathol 26 (8) 862-865.
Zborilova B, Oborna I, Tkadlec E, Prochazka M, Breziniva J, Sobek Jr A, Sobek A (2018) Does EmbryoGlue transfer medium affect embryo transfer success rate? Ceska Gynekol 83 177-181.
Zorn TM, Pinhal MA, Nader HB, Carvalho JJ, Abrahamson PA, Dietrich CP (1995) Biosynthesis of glycosaminoglycans in the endometrium during the initial stages of pregnancy of the mouse. Cell Mol Biol 41 97-106.
Gkotsi, A, Makri, D, Maalouf WE (2021) A systematic review on the clinical efficacy of EmbryoGlue in implantation outcomes. Fertility 2021 Online (P104).
*Vitrolife, data on file
Topics: Embryo culture & transfer